Infectious diseases exert a large burden on the well-being of human societies, as vividly illustrated by the recent COVID-19 pandemic. In response to an infectious disease, governments enact a variety of non-pharmaceutical interventions (NPIs) such as social-distancing guidelines, mask-wearing mandates and lockdowns. These NPIs reduce spread of the virus causing the target disease, and also reduce spread of other viruses that cause non-target diseases. For example, NPIs enacted during the COVID-19 pandemic reduced the spread of non-target respiratory diseases caused by influenza and respiratory syncytial virus (RSV). However, due to lack of pharmaceutical interventions aimed at these non-target diseases (such as vaccinations), they often rebounded to levels higher than pre-pandemic levels after the NPIs were relaxed. Thus, the net effect of NPIs on the long-term total disease burden of non-target diseases is unclear.
This knowledge gap was addressed in a new study by Tak, Ryan and Jonah Goh (former Honours student at Chisholm Lab), recently published in the Journal of Theoretical Biology. We considered a scenario where NPIs were enacted for a year and then completely removed. Under this scenario, we analysed a suite of four epidemiological models of varying generality and complexity, to quantify the net effect of the NPIs on the long-term total disease burden of a seasonal, non-target respiratory disease.
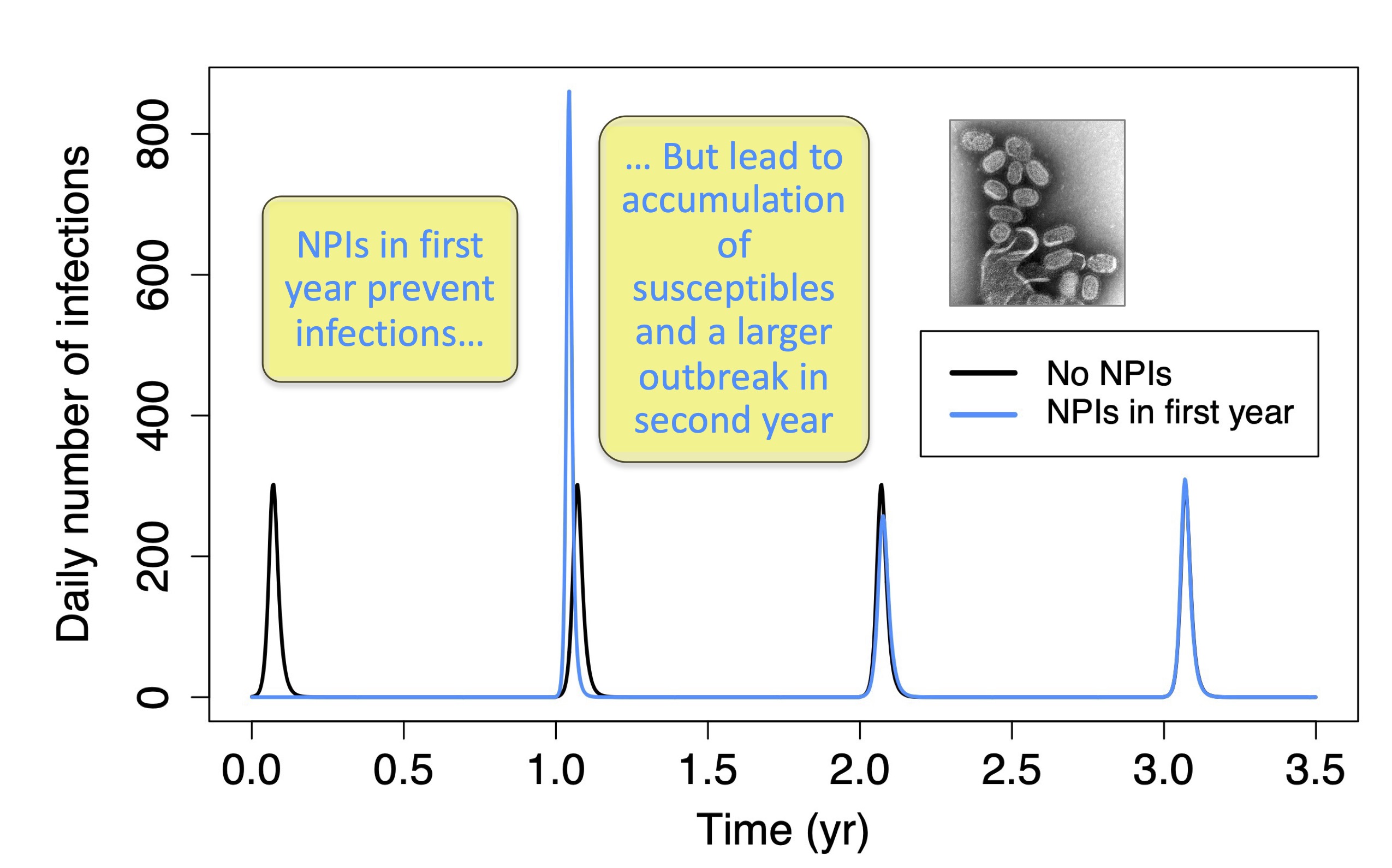
The simplest model of the four was a SIR model with seasonal disease outbreaks and temporary immunity of recovered individuals. For this model, we performed a rigorous mathematical analysis to show that the net effect of NPIs was always to reduce the long-term total disease burden. The number of susceptible individuals increased during the year when NPIs were enacted and this led to the number of infections rebounding to high levels after the NPIs were removed (Fig. 1). But this was more than offset by the number of infections prevented by the NPIs when they were being applied (Fig. 2). We found that the net reduction in the number of infections depended critically on the rate at which immunity was lost. In the extreme case of near-permanent immunity, the pool of susceptible individuals remained small and resulted in small outbreaks, such that the NPIs produced a small net reduction in the number of infections. However, as immunity was lost more quickly, the size of outbreaks increased commensurately and the NPIs produced increasingly larger net reductions in the number of infections, with the net reduction reaching large values of 70-100% of population size when immunity loss occurred quickly (on the order of months).
These key results from the simplest model were supported by simulations of the three more-complex models, which were parameterised for specific locations including Singapore and China. Overall, our study highlights a hitherto under-appreciated role of NPIs in reducing the long-term total disease burden of non-target diseases, which should be factored into cost-benefit assessments of NPIs in public health management.